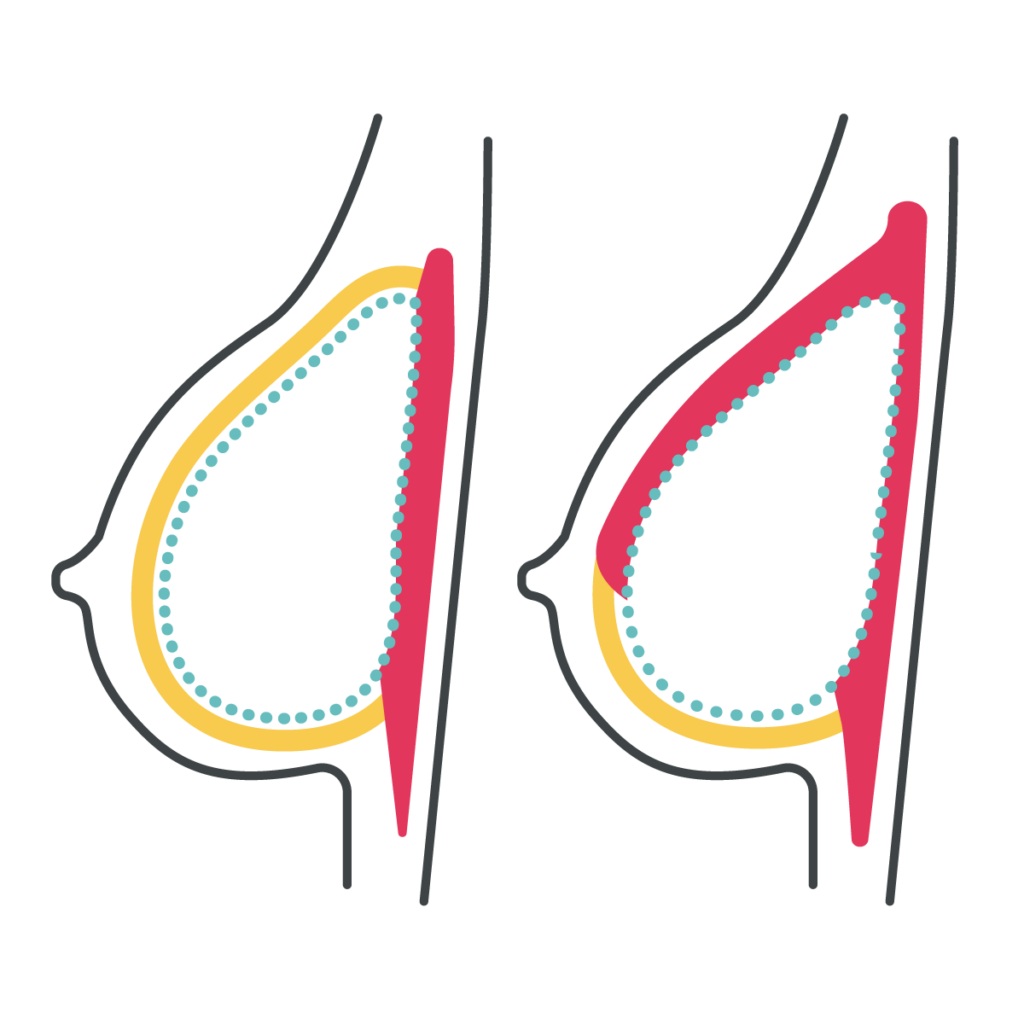
Pros: Under-the-muscle implants are a more familiar technique for many surgeons, based on their prior training. Patients are less likely to have rippling or visible edges of the implant along the top of the breast, and potentially can have better screening for future recurrence if the cancer is right on top of the chest muscle.
Cons: With under-the-muscle implants, patients can experience more short- and long-term pain, and frequently have “hyperanimation deformity” along the top of the breast with pectoralis movement. In addition, the implants are often displaced towards the armpits/sides or appear flattened along the top.